Anesthesia Robot Remote Platform
A web platform enabling anesthesiologists to remotely monitor and control intelligent anesthesia robots across multiple simultaneous surgeries in real time.
China’s anesthesiologist shortage
meets a robotic solution
Ratio of surgical demand to available anesthesiologists, widening with aging demographics.
Core proposition: one doctor supervises multiple robot-assisted surgeries remotely.
Missed command tolerance is effectively zero in remote infusion control.
The design challenge
The robot automates drug delivery, but the anesthesiologist must remain in control for critical decisions, anomaly response, and emergency interventions.
The UX challenge: provide full situational awareness and trusted remote control across cloud infrastructure, without latency ambiguity or cognitive overload.
The platform also acts as a nationwide patient record system with strict privacy, role-based access, and full audit traceability.
Understanding target users
Dr. Zhang — Anesthesiologist
PRIMARY USER“I monitor multiple surgeries at once. I need instant awareness if any case deviates.”
- Real-time visibility of vital signs across concurrent sessions
- Fast, trusted remote drug adjustment workflows
- Clear normal-vs-anomalous visual states
- Immediate connection loss visibility
- Cognitive overload when monitoring in parallel
- Latency anxiety between command and pump response
- Record retrieval friction across systems
Liu — Platform Administrator
ADMIN USER“Account access has to be precise and revocable immediately, with full accountability.”
- Permission governance with audit logs
- Rapid access revocation and role reassignment
- System-wide visibility of sensitive actions
- Manual account workflows are brittle
- Permission states are hard to inspect
- Deletion/edit actions lack guardrails
Wang — Data Maintainer
SECONDARY USER“I need to correct records safely without touching legally protected intraoperative data.”
- Clear editable vs read-only field boundaries
- Safe confirmation for data edits
- Patient lookup with minimal friction
- Editability ambiguity in existing systems
- Weak per-record history visibility
- Overly strict search field burden
Synthesized User Needs
Critical Pain Points
Understanding how the
anesthesia robot actually works
Interface decisions came from system behavior. I studied drug-delivery mechanics, command routing, and surgical protocol dependencies before finalizing interactions.
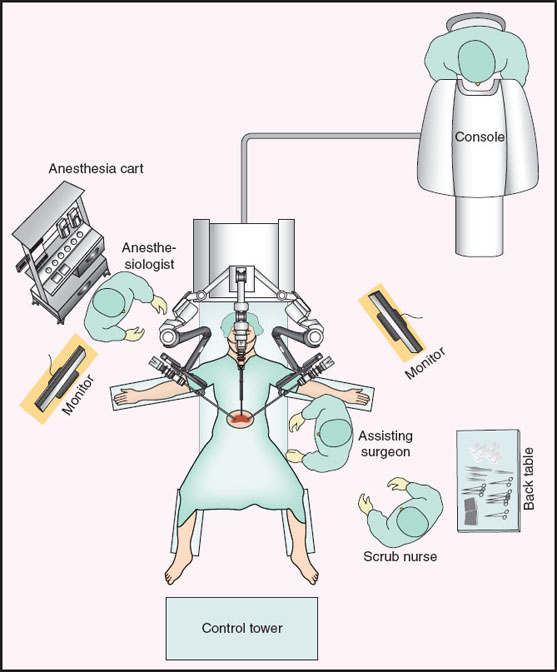
The robot’s role in surgery
The robot continuously monitors vitals and adjusts infusion rates to maintain target anesthesia depth. The doctor remains responsible for intervention and clinical decisions.
Local Machine
Collects vitals, runs dosing logic, controls pumps directly.
Cloud Server
Stores data, routes commands, enforces role-based access.
Web Platform
Doctor-facing UI for live monitoring and remote intervention.
Critical constraint: Web UI → Cloud → Local machine → Pump must confirm each command stage.
Induction
Rapid transition to anesthesia depth. Highest risk period.
Maintenance
Primary remote monitoring phase with AI adjustment.
Recovery
Drug tapering and post-op risk observation.
Mapping the system
Information Architecture — Frontend
Auth
- Login
- Register
- Password reset
Dashboard
- Surgery metrics
- Recent patients
- Quick actions
Database
- Search
- Patient profile
- Vitals and logs
Remote
- Session hub
- Live monitoring
- Pump controls
| User Type | Patient Data | Edit Records | Remote Control | User Mgmt | Export |
|---|---|---|---|---|---|
| Anesthesiologist | Own hospital | If granted | If granted | ✗ | If granted |
| Data Maintainer | Own hospital | Non-surgical only | ✗ | ✗ | If granted |
| Administrator | All hospitals | All records | ✓ | ✓ Full | ✓ |
Three critical flows through
the system
Close recreation of the flow intent, presented in three parallel flow maps.
Authentication Flow
Database Lookup Flow
Remote Surgery Flow
User journey
Six key screens across the full flow, with rationale aligned to critical UX constraints.
Login
Role-aware split entry with clear accountability.
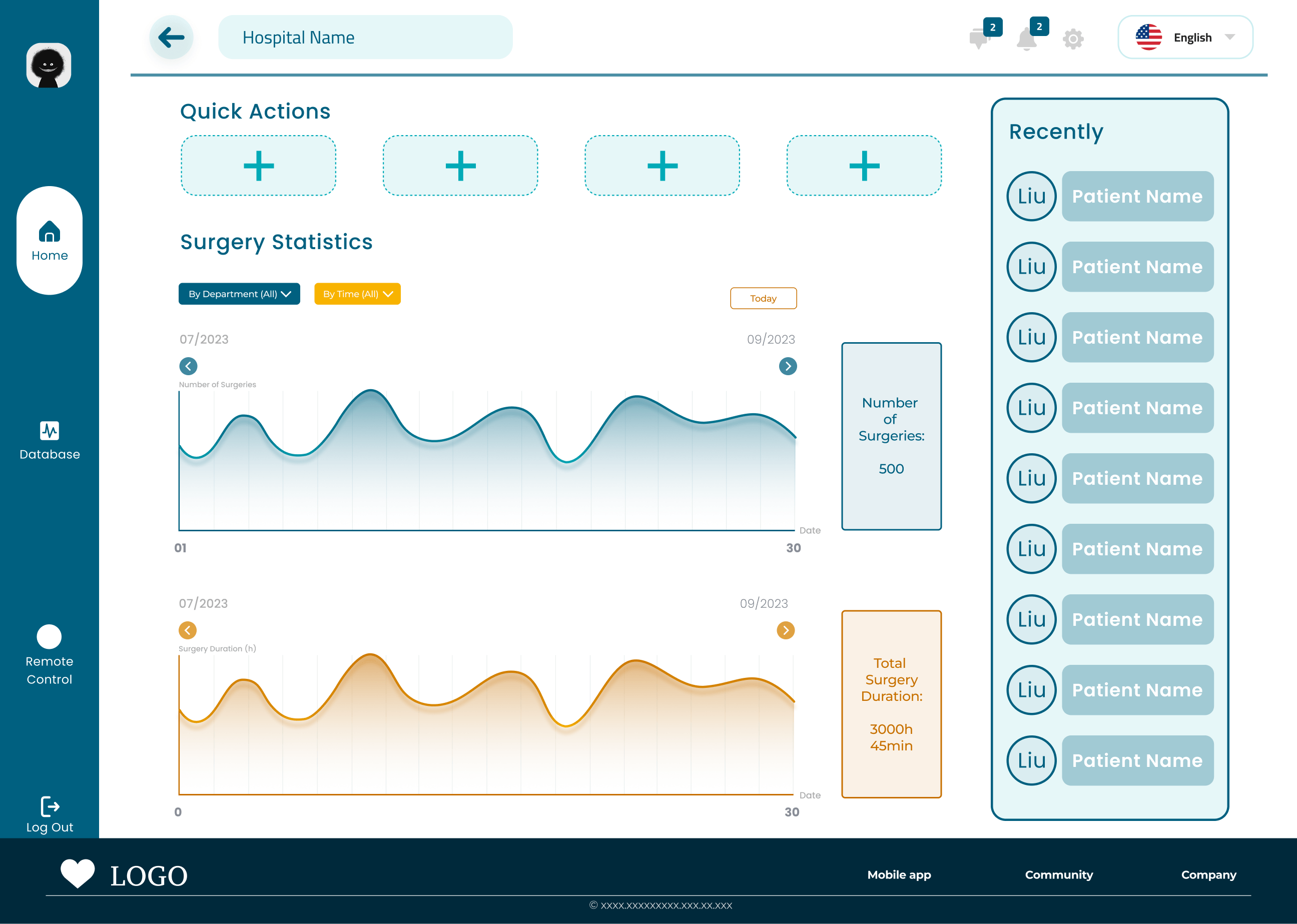
Home Dashboard
Workload and trend visibility with quick patient re-entry.
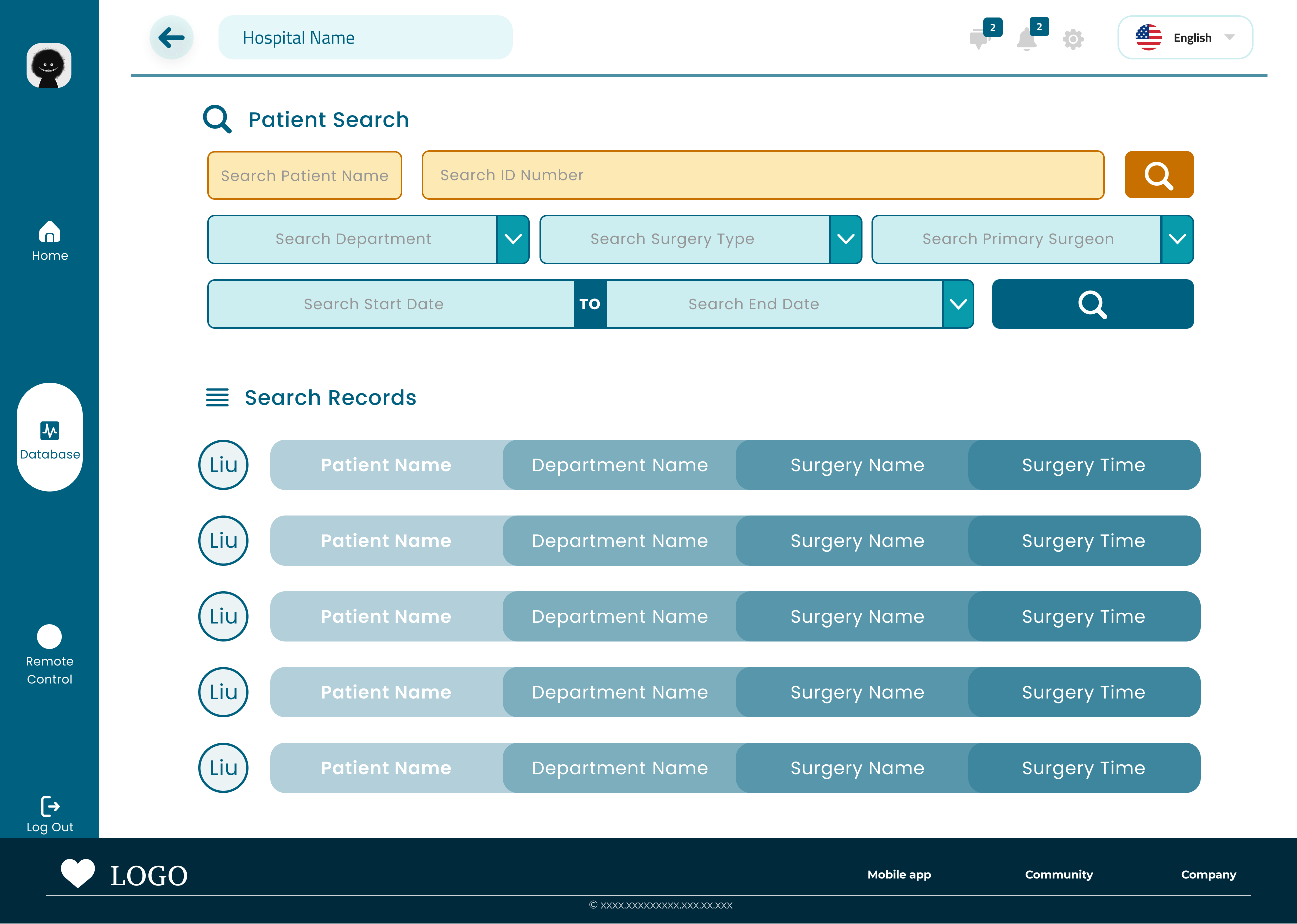
Patient Search
Privacy-first retrieval with fast path and filters.
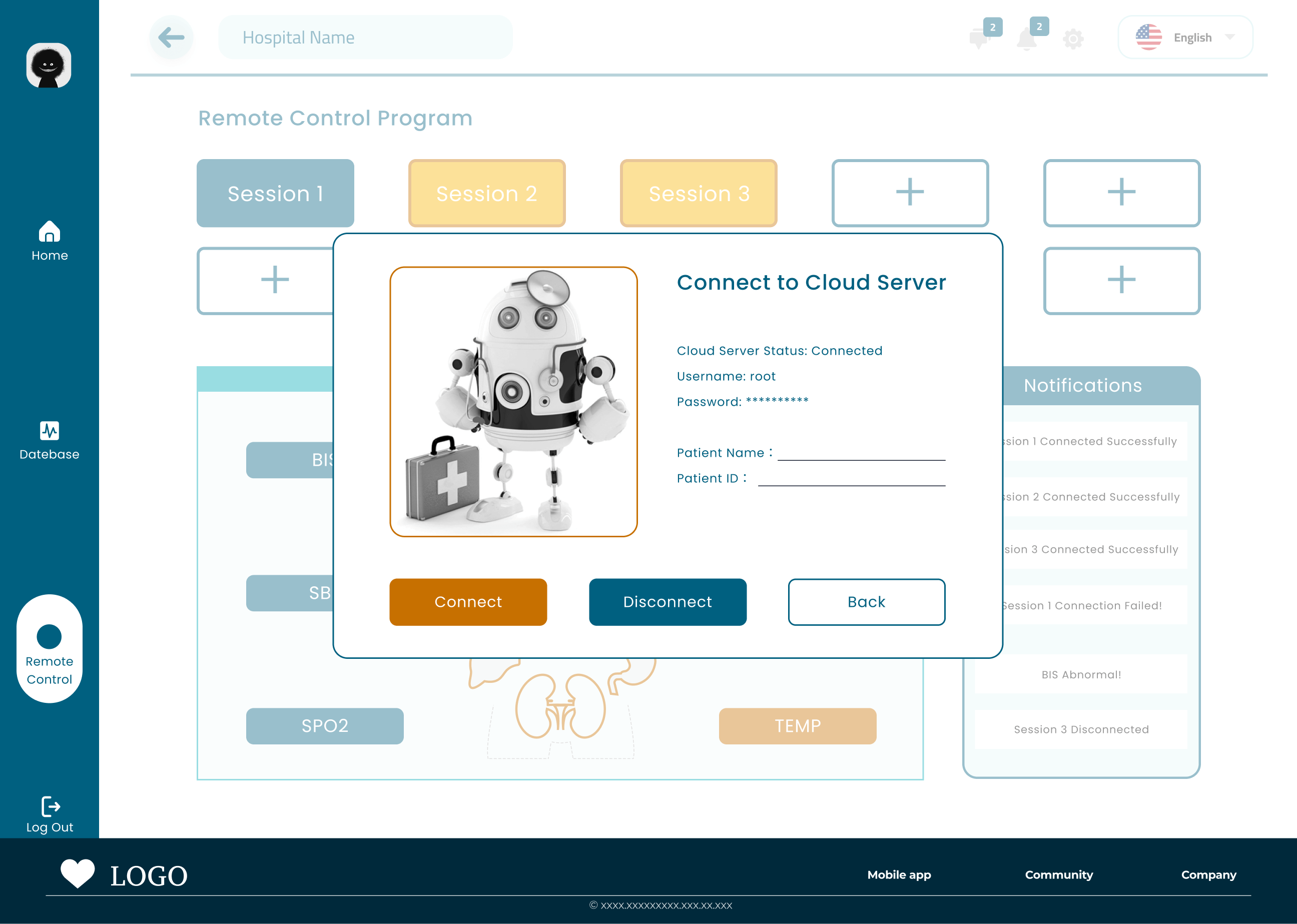
Remote Control Connecting
Connection setup and verification before entering active control.
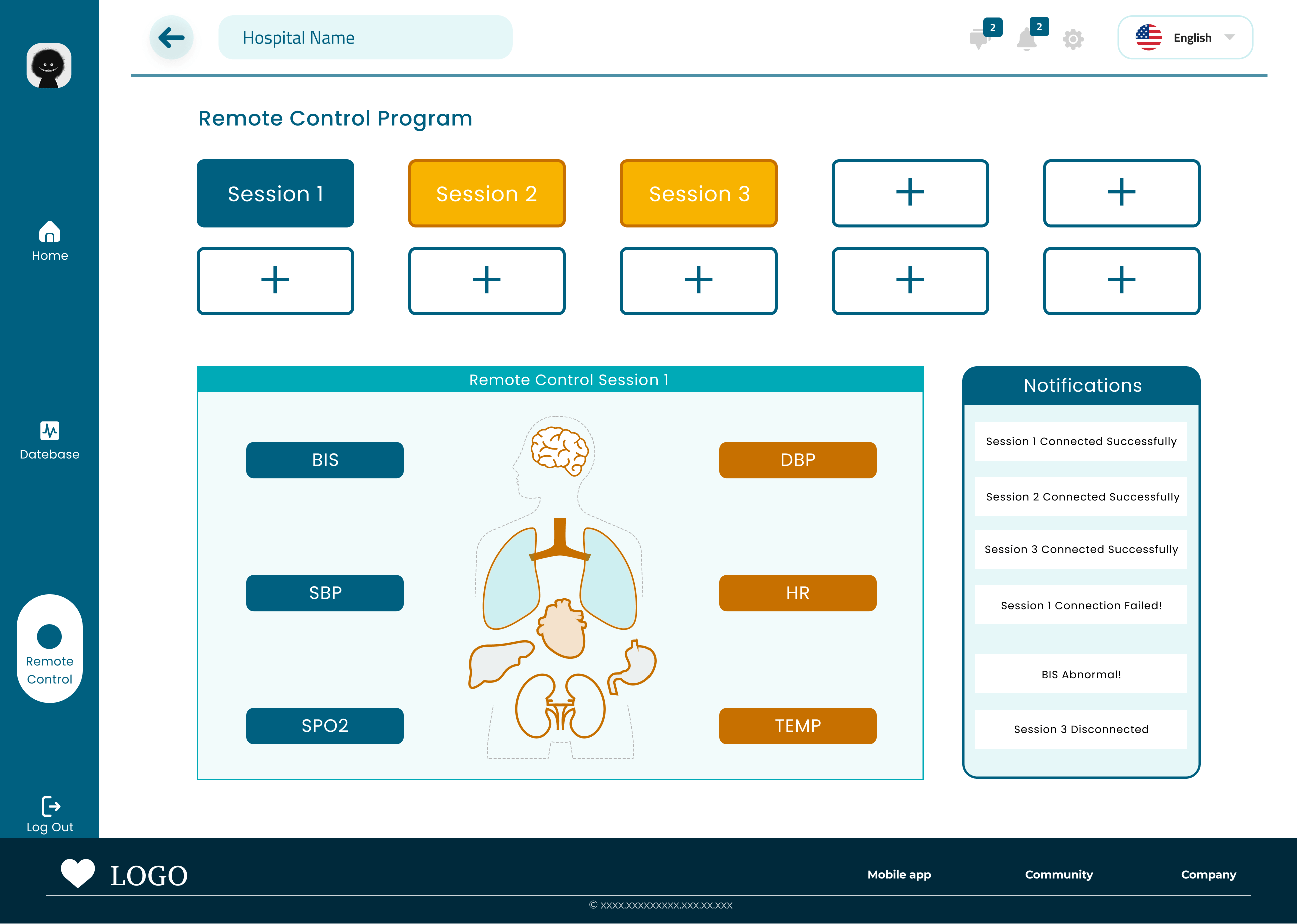
Remote Control Hub
Grid-first parallel session management and notifications.
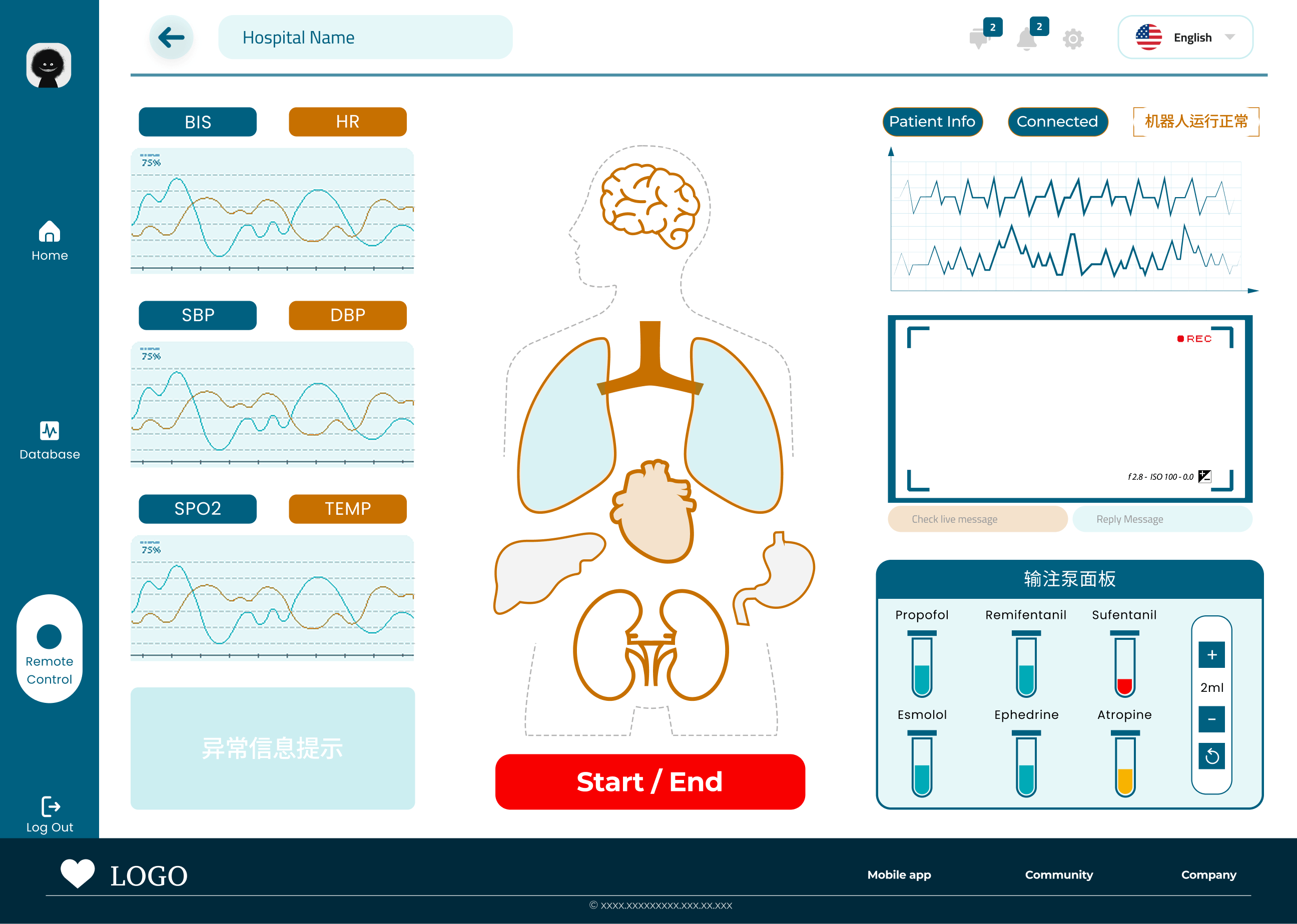
Active Session
Maximum-density command and monitoring environment.
Try the prototype
What I’d do differently,
and what comes next
Usability testing with anesthesiologists
Validate time-critical interactions and confidence in remote dose adjustments.
Emergency flow completeness
Network drop, pump failure, and severe-state response flows need full coverage.
Domain fluency shapes layout
Clinical understanding changed system structure, not just labels.